 |
| Dr Sarah Goldsmid, surgeon at the Animal Referral Hospital in Sydney. |
Veterinary surgery can be extremely rewarding, but it can also be extremely challenging. Surgical specialists take on the really tough cases. Dr Sarah Goldsmid, based at the Animal Referral Hospital, is one woman who has carved out a career at the cutting edge. Not only can she perform surgery that many others won't - she often gets out of bed in the middle of the night to do it. She's the kind of person we want to be when we grow up. But she was still happy to chat to SAT about her career.
It is often said that some people are born surgeons. So were
you naturally good at tissue handling from the get go, or did you have to work
on this?
I think it is true to say
that good surgeons naturally have a reasonable amount of dexterity and
creativity. I loved craftwork when I was young – especially needle work. I was
good at making things with my hands and I think that is a good skill to start with.
As far as dealing with body tissues – you need to be confident in your
anatomical knowledge and you need to practice, practice, practice. Watching
gifted surgeons at work is also an inspiration in how to handle tissues, hold
instruments, retract and follow Halsted’s surgical principles.
There must have been a
certain level of natural surgical skills, because I remember my first live dog
spey when I was in 4th year vet science (at Sydney Uni Camperdown).
I did the procedure in ½ hour and it went really well. The surgical registrar
was impressed and told me I was going to be a surgeon …. she obviously knew
more than me at that stage. I hadn’t even considered specializing and had no
idea what was involved.
 |
| Sarah performs surgery on a dog with a GDV (gastric dilatation volvulus). |
How did you improve and hone your surgical skills?
I have already partly
answered this, but certainly practicing procedures is important. I learnt
quickly and once I had done a procedure even just a couple of times, I became a
lot more confident. As a surgical resident, the specialist surgeries were
learnt by firstly watching specialists do the surgery at the university as an
assistant. Then I would perform the surgery with a specialist assisting me.
Finally I was let loose on patients without my hand being held. I paid close
attention to any tips or pointers that other surgeons would give (some I found
useful, but not all). I also tried to attend as many conferences on surgery as
I could and even better if there was a practical component in the course.
 |
| Performing an L7-S1 laminectomy in a dog. |
Specialist surgeons appear to tackle anything with ease. How
much planning goes into your surgical approach? What procedures take more
planning than others?
Any surgery requires
planning. You need to consider your surgical approach, options when you are in surgery
(always have a plan B and maybe a plan C and D as well), have an understanding
of possible complications that might occur during surgery and postoperatively
(and have a plan of how you would manage those complications if they arose).
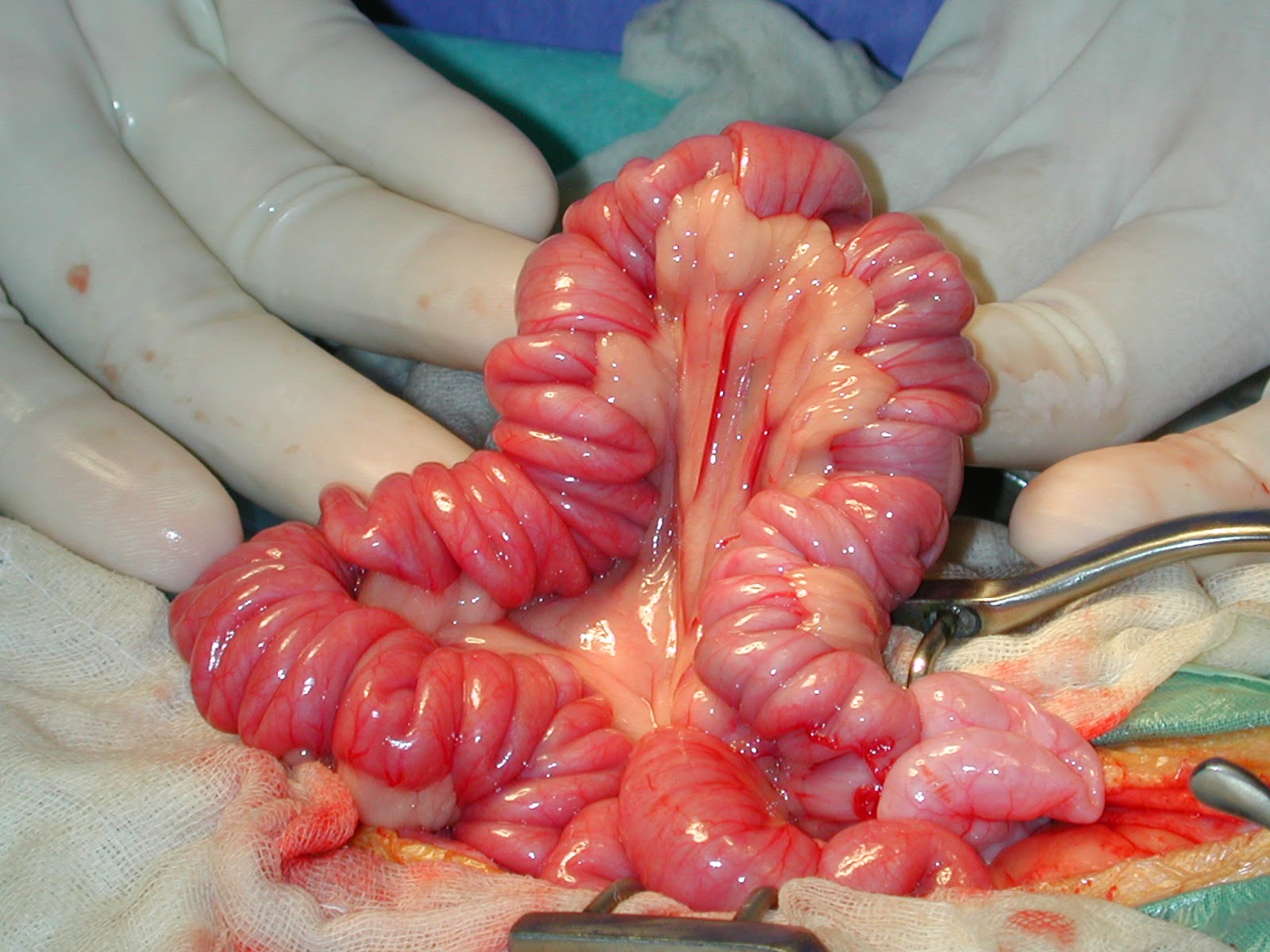 |
| A linear foreign body. Note the plicated intestine. Definitely a surgery you need a plan B, C and D for... |
While some procedures
that we do regularly do not require so much thought – some of the more unusual
procedures require a lot more planning.
For instance – some of
the mandibulectomies or maxillectomies to remove oral cancers are planned by
creating 3D reconstructions of the lesion and skull from our CT images.
Difficult fracture repairs can be likewise planned on reconstructions or using
templates. For corrective osteotomies we might have the implants pre planned
and pre made (such as Type II or III or Ring External Fixateurs).
Reconstructive surgeries require a detailed understanding of skin flaps and
grafting techniques. It is an artform (much as a sculptor plans in 3D) to
create an appropriate flap from adjacent skin or move a free flap from another
part of the body (carefully trying to match colour, hair type and hair
direction) to end up with a cosmetic and functional result. Spinal and brain
surgeries require careful planning to ensure an approach that is minimally
traumatic and gives the best access to the site of the problem – usually with
the aid of an MRI.
 |
| Pre-operative MRI aids planning. |
Did you have any surgical mentors and heros/role models when
you were training?
My two main mentors were
Dr Chris Bellenger (particularly in soft tissue procedures) and Dr Ken Johnson
(mainly orthopaedics). During my time as a resident at Sydney University, I was
also lucky enough to be exposed to at least another 6 Boarded North American
surgeons who visited and worked at the uni during the time I was there. It was
like visiting all the major veterinary university surgical services in the USA
– but they came to me. That doesn’t happen now and I think it was a wonderful
learning experience for me.
 |
| Am I easily impressed...or is this the most impressive prostatic cyst you have ever seen? |
What is your favourite surgery to perform and why?
That’s a hard one to
answer, because I get a thrill from any surgery that goes well and the owner’s
and patients are really happy. I love seeing a spinal patient (that was carried
in to the consult) walk out the door to go home – that is a great feeling. I
love hearing from the owner that their dog has become like a puppy again since
I removed the chronicly infected ear canal with a total ear canal ablation and
lateral bulla osteotomy. I find it really rewarding to see a dog walk and run
after their fracture was repaired, or their cruciate ligament deficient stifle
was stabalised. It is so rewarding when a dog with cancer can be successfully
surgically treated and be cancer free, or a cat with 3rd degree
burns to all 4 feet can be managed to have fur regrow on all feet and walk, run
and jump again.
I think what I really
enjoy about being a specialist surgeon is the huge variety of cases and the
unexpected and unusual cases.
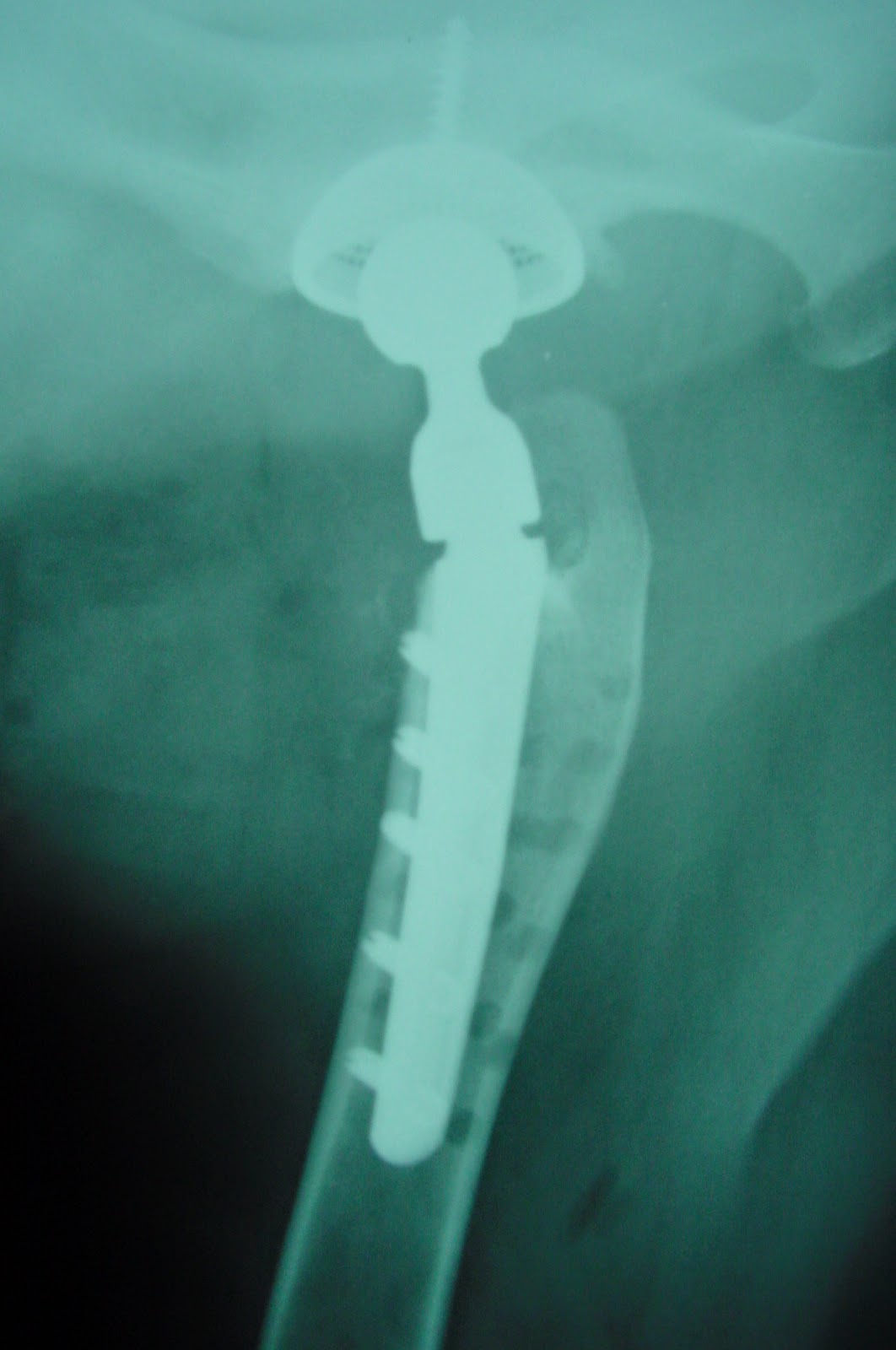 |
| Total hip replacement in a dog. |
What surgeries do even specialist surgeons find challenging?
> or what is your LEAST favourite surgery?
It is always a little
challenging to be the second surgeon to perform the procedure. So, for
instance, when someone has attempted resection of a cancer and has placed a
drain several centimeters from the original mass – so you are forced to remove
not only the original mass with a margin, but all the drainage tract with a
margin as well. Or, having to reconstruct a fracture that is infected and has
unstable implants already placed – that can be a little challenging.
I think the most
frustrating cases are those that if you had only seen them a little earlier –
the prognosis would have been vastly better. So particularly things like acute
spinal cases, due to herniated intervertebral discs, that lost deep pain more
than 24 hours ago ….. if you had just seen them a couple of days earlier the
prognosis may have been 85-90 per cent chance of walking again (while they still had
deep pain) vs less than 10 per cent when they have lost it for more than 24 hours.
 |
| Sarah works with a dedicated team. |
Complications occur in medicine and surgery. What is the most
challenging complication you've ever dealt with?
When doing a PDA (patent
ductus arteriosus) surgery – the biggest concern is the vessel you are trying
to ligate may tear and the puppy will bleed out in a very few seconds,
particularly when they are often only a kg or two in weight. Naturally you are
thinking about this while carefully dissecting around the vessel and placing
the suture.
I remember one such surgery, right at the critical point when I was
just passing the suture around the vessel – the surgical intern who was
assisting me passed out and fell backwards. The vessel tore, the puppy started
to bleed out and I quickly managed to get the suture around the bleeding vessel
and tie it to stem the blood flow. Meanwhile yelling for someone to come and
assist my intern while the nurse managed the anaesthetic. Both intern and puppy
did well after the ordeal. My heart beat a little faster for a while.
 |
| A good surgeon is calm under pressure. |
What character traits are desirable for a career in surgery?
I know I am female – but
I often say you have to have “balls” to be a good surgeon. That is to say – you
need to be confident, bold and definitive. It’s no good being really gentle,
slow and hesitant. So when the bone is bleeding dramatically while you are
sawing away part of the maxilla – you have to keep going because you cannot
control the bleeding until you have the jaw removed and you can access the
origin. When you are doing cancer surgery, you have to remove the cancer with a
margin of normal tissue, in other words you have to be bold and make a damn big
hole. Then you have to have a plan (or maybe two or three) of how to deal with
the big hole.
To even get to be a
surgeon you have to have perseverance, discipline and be prepared to work hard
(day and night).
It is probably not the
best career to choose when you are a mother – having said that I have
successfully had two children and raised them to adulthood. Neither of them
have become axe murderers, yet. I couldn’t have done what I do without a very
supportive husband. It is tough to be working long days, trying to run away at
the end of the surgery to pick up a daughter from childcare when they are
charging you $8per minute you are late. Or getting called out in the middle of
night, then rushing home to get them up to get to school, remembering the
school project, gym clothes, softball bat and violin …. you get the picture. It
can be done, but you have to be organized, resilient and have a sense of
humour.
 |
| A surgeon's view... |
What is the difference between a good surgeon and a great
surgeon?
Communication skills. You
can be the best surgeon in the world, but if you can’t communicate with your
clients to explain the procedure, prognosis and complications in understandable
terms and appear confident – then no owner will want you to operate on their
pet.
Of course you have to be
able to deliver on the surgery as well.

 Anne Fawcett 2014")

 Anne Fawcett 2014")




 Anne Fawcett 2014")

 Anne Fawcett 2014")
 Anne Fawcett 2014")










